Gluteus Maximus Transfer Surgeon

Do you have a long-standing or chronic gluteus tendon tear, failed gluteus tendon tear repair, or irreparable and atrophied (shrunken) gluteus tendons/muscles? If so, a gluteal repair is nearly impossible. These types of injuries, tears or conditions require a gluteus maximus transfer. Doctor Ronak Mukesh Patel, provides diagnosis as well as surgical and nonsurgical treatment options for patients in Houston, Sugar Land, and Pearland, TX who have irreparable or long standing gluteal tendon tears that were previously inoperable. Contact Dr. Patel’s team today!
What is a gluteus maximus transfer?
A gluteus maximus transfer is done for chronic or long-standing gluteus tendon tears, failed gluteus tendon tears, or irreparable and atrophied (shrunken) gluteus tendons/muscles. In these cases, gluteal repair is made nearly impossible. These types of injuries, tears or conditions require a gluteus maximus transfer. Dr. Patel does a gluteus maximus and tensor fascia latae transfer (TFL). This can also be done for patients with a prior total hip replacement or during the same setting as a hip replacement for the same problem. Dr. Patel will sometimes work as a team with a total hip replacement surgeon to do these cases. The goal of a gluteus maximus transfer is to minimize the symptoms, stabilize the hip and pelvis, improve walking, and restore gluteal strength and function.
What is the gluteus maximus?
The gluteus maximus or “Glutes” in layman terms, is the “sitting muscle” or the part of the buttocks that you sit upon and the muscle that helps the body stand or sit easily. The gluteus maximus is the most superficial and largest of the three gluteal muscles and makes up the bulk of the shape and form of the buttock and hip area. The gluteus maximus is quadrangular in shape and slopes across the buttock at approximately 45 degrees to its distal insertion. The job of the gluteus maximus is extension and external rotation at the hip joint. The gluteus maximus is important for powerful lower limb movements like stepping onto a step, climbing, or running.

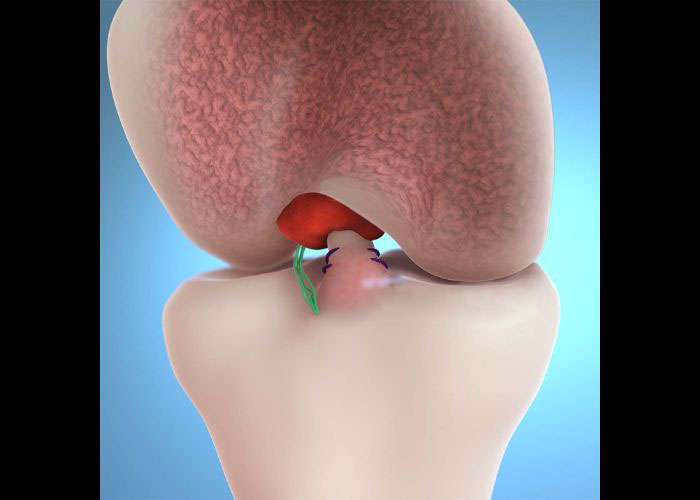
How is a gluteus maximus transfer done?
Dr. Patel typically does this procedure with an open incision. He creates a surgical incision over the side of the hip and extend it proximally and posteriorly toward the posterior superior iliac spine. Electrocautery is used to dissect down to the iliotibial tract. In this technique, the anterior portion of the gluteus maximus and the posterior portion of the TFL are located and moved to the greater trochanter so that that the muscle fiber direction of the transferred muscles closely matches that of the gluteus medius and minimus. Dr. Patel uses this to create a substitute for the deficient gluteus (abductor) muscle. He ensures a tight repair by attaching the flaps and tensioning the abduction. This creates a “new” gluteus tendon that will perform the functions of the original muscle.
What is the recovery like for a gluteus maximums transfer?
The recovery process for patients undergoing a gluteus maximus transfer can vary based on prior health and surgeries, age, strength, and underlying conditions. In general, patients can expect the following:
- Adduction and abduction are not allowed for the first 6 weeks.
- Only flat-foot partial-weight bearing is allowed (20 pounds max) with assistance of a walker or crutches for 6 weeks.
- Patient will wear a hip abduction brace.
- Hip flexion is limited to 0-90 degrees.
- Active hip abduction and internal rotation should be avoided for 6 weeks
- Passive external rotation and passive hip abduction should be avoided for 6 weeks.
- Slow progression to full weight bearing starts at 6 weeks with physical therapy using a specific protocol developed by Dr. Patel
- Strength and range of motion will improve over 6 to 8 months.
- Total recovery time is 6-12 months.